
Whether your clients have complained about it being tight or you’ve experienced it firsthand, the IT band is searched popularly on YouTube and commonly among those who exercise regularly. Aside from discussion, there is plenty of debate on how to manage tightness or injury, most specifically on how to handle IT Band Syndrome.
Should we foam roll or should we not? To answer this question and to address this common complaint with our clients, we can start by better understanding this thick band of connective tissue, what it is, and how it works.
What is the IT band?
The iliotibal band (IT band or ITB) is a thick band of connective tissue that runs along the outer thigh from the hip to the knee. The largest piece of fascia in the human body, it is formed at the hip by the fascia of gluteus maximus, gluteus medius, and TFL (tensor fasciae latae). It’s insertion at Gerdy’s tubercle means it has no bony attachment which allows it to move anteriorly and posteriorly with knee flexion and extension.
Though its function is typically considered to be pelvic stabilization and posture control, the ITB is an important structure involved in motions like walking and running. It is involved in hip extension, hip abduction and lateral hip rotation.
In studying the IT band, researchers found its elasticity and structure is similar to that of the Achilles tendon. This suggests that it does not just aid in the movement during running, but could also be important in saving energy.
Dysfunction and Injury
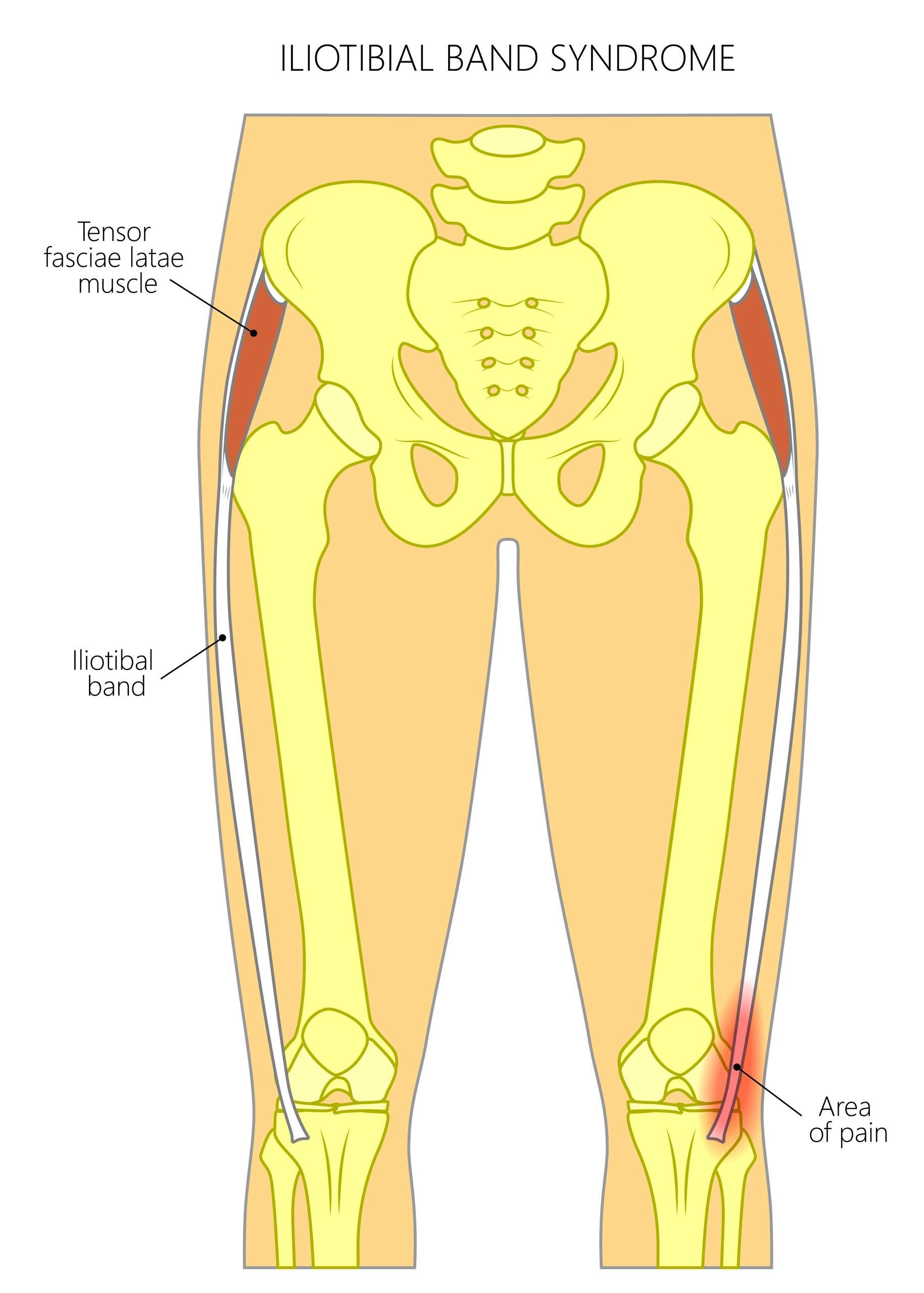
Because of its involvement in actions like running, its dysfunction presents as a common injury found in runners: IT Band Syndrome. This Syndrome is considered a knee injury, where the pain typically presents, and is a non-traumatic, overuse injury. In many cases, there is an underlying weakness of hip abductors. Chronic inflammation of IT band bursa is also a contributing factor.
Another known pathology is external snapping hip syndrome, characterized by a snapping sensation and/or sound in or around the hip during movement.
Aside from injury, the ITB can often feel tight on individuals. Whether or not there is hip or knee pain present, you or your clients may have experienced this feeling of tightness and feel the need to stretch or massage the area.
Should we foam roll IT Band?
A commonly debated topic is whether or not we should foam roll the illiotibial band. You may see people at the gym foam rolling their outer thigh, or you may have tried it and found that it provides relief after a workout or a run.
You may wonder why some will argue we should never foam roll the IT band, especially if you have experienced the temporary relief foam rolling can provide. Well, that’s exactly why; the relief is only temporary.
While it may not be damaging to use SMR techniques on this tissue, it is also not addressing the root of the problem: Because it is fascia, not muscle, foam rolling will not break up scar tissue, soften muscles or release tension.
When foam rolling to address discomfort related to the IT band, it makes more sense and is more effective to roll the muscles it is attached to: the vastus lateralis, the glutes, and TFL.
My take? All of these are fantastic tools, but a smart trainer uses the right tool at the right time….and on the right spot. But foam rolling over your IT band is, frankly, a bad joke nowadays. Why? Well, let’s get into the anatomy to find out!
Anatomy of Leg and Hip Musculature
The IT band, or iliotibial band, is just a thick band of connective tissue that acts as a lateral stabilizer, connecting the big outer ridge of our ilium to our tibia, (just below the knee joint, laterally). Embedded at the top of the IT band, functioning as a tension moderator, is our lovely little TFL, or tensor fascia latae, meaning “Wide fascial tensor”. The TFL is a muscle despite the word “fascia’ confusing matters, but its insertion flows seamlessly into the fascia of the IT Band.
Fascial considerations, or rather, other structures that can tug at this band via the fascial highway or direct connections include the obliques, the glutes, the peroneals (fibularis group) on the lateral calf, and of course, the lateral quad muscle, the vastus lateralis. Yes, the super-mega-big-giant-huge-colossal muscle that sits immediately under the IT band could possibly-maybe-perhaps play a super-mega-big-giant-huge-colossal role in the functioning of this band.
Common Treatments for ITB Troubles
Foam rolling seems to be a go-to as far as IT band pain is concerned, at least over this tissue itself. As a tool, foam rolling really only improves fluid dynamics and exerts a mild neurological stimulating effect on areas rolled over. As the pressure from the curved surface digs across our tissues, the roller essentially bull-dozes superficial fluids (blood/lymph) out of the way, and a wake of negative pressure is left, pulling in newer blood flow to fill the space.
Rolling over the band itself would be considered overkill, not to mention very painful. When we’re in pain, things tighten up. I’d argue here that there’s no point to causing more tightness and pain in a tight and painful area that really is just thick connective tissue, which requires no significant blood flow to function.
The gurus that claim to have solved IT band syndrome are certainly on the right path. Each, in their own way, comments on using the roller more specifically, targeting the bellies of the muscles actually responsible for the IT band. These include rolling or lacrosse-balling on the aforementioned TFL muscle, glute max, and gluteus medius. Excellent thinking here, and certainly more effective than the prior option.
Other practitioners, including Chiros, PTs, and ATCs, might blame mechanics. IT band syndrome is, by its nature, an overuse injury, and their thinking here is that if your hip is not tracking properly through a stride (either too much external or internal rotation), then the IT band no longer acts as a stabilizer, but forced into part-time labor as a compensational hamstring or quad fiber.
This causes more irritation and rubbing at the knee joint, and BAM…Syndrome Town…population: You.
More discerning practitioners will help to isolate the issue; sometimes lack of mobility or strength at the hip, other times lack of strength or mobility at the knee, ankle, or even big toe can be to blame. There are about a thousand ways to fix these biomechanical issues and most of these approaches have great outcomes.
A Functional Perspective
It’s not your IT band. It’s your vastus lateralis. Take a deep, long look at any anatomical depiction of the IT band and then match it with a deep, long breath, for you have now seen the light! When we complain about the IT band, we’re typically referring to chronic repetitive stress occurring at or around the lateral knee, which translates to a tension issue.
When we then track back to find the muscles that control the tension at the lateral knee, we discover the TFL/Glute complex and can easily address those particular muscles in our favorite ways. This might help a lot, but does the problem go away completely? Likely not.
There’s a reason why those muscles are staying tight: they’re also overused and compensating for improper biomechanics. But why are the biomechanics improper?!?! My assertion: Adhesion between the IT band and lateral quad are playing tug-of-war, and guess who’s losing?
We know both overuse and underuse can cause adhesion. In the case of the office worker seated for eight hours a day, underuse is the cause. In the case of a marathoner, it’s overuse. Any mix of those two could yield the same outcome, as well. If we look at this IT band issue from the beginning, it starts to make more sense:
Sitting + Time = Adhesion
Weekend Warrior Activity (Or Sport) + Time = More Adhesion
Adhesion + Movement = More Adhesion, Tight Muscles, and Aberrant Biomechanics
IT Band + Lateral Quad Tug-Of-War = Pain and Angry IT band
Is There An Easy Fix?
Now that you have a better idea of the etiology of this tightness at the IT band, you’ll have a better path to success with reducing the tension and irritation. My goal is always to get it gone 100%. Since we’re dealing with adhesion, mobility work is really the key. As a sports chiro, I’m allowed to have my hands on people, using soft tissue techniques like ART or MRT, Graston or IASTM, and Cupping to help my clients to find relief, but as a personal trainer, you might not!
Training Considerations
Because IT Band Syndrome is such a common injury, it’s something we should have a basic understanding of as trainers, especially if we work with more susceptible athletes like runners.
As always, in cases of injury we would need to follow doctors’ recommendations. But when we know someone we are working with performs activities like running often, we can work to prevent IT band pain by incorporating exercises that strengthen the hip abductors, and include stretches and foam rolling for the hip muscles in cool down and recovery.
My strong suggestion for IT band pain relief: Banded flossing, the application of a narrow latex band wrapped around the limb, is a great way to help get past the pesky adhesions, and after that, it’s as simple as calming down the leftover tightnesses in the TFL and Glutes. (A lacrosse ball or foam roller will certainly do the trick to release trigger points or adhesions in the muscle bellies).
The floss compresses the IT Band and Quad together and puts a greater strain on the tug-of-war action. The safe bet here is that the adhesions themselves break up without further irritating the quad or ITB. I typically will do some activities like my squat “shapes”, as I demonstrate in the video, to shear those tissues for about 2 minutes, maybe twice, before getting out the roller or lacrosse ball and doing some compression work on TFL or Glute Med/Max for 20 seconds, three times per spot.
Then I roll my IT band…JUST KIDDING.
But a pro tip here is to roll the anterior AND posterior aspects of the lateral quad without squashing your ITB. I do this by internally or externally rotating my thigh while I’m also rolling my quad and hamstring, respectively.
Here’s my ITB Tightness Alleviation Protocol:
1. Banded Flossing – 2 min x 2 sets – Any functional IT band motion or exercise, pick your favorite (Squats, treadmill, single leg functional reach, etc.) while wearing the flossing bands. Test between sets. ~ 5 min
2. Lacrosse Ball Release– 20-second reps x 3 sets per area – Hit TFL, Glute Med, Glute Max, and even Vastus Lateralis if you want! ~ 2-3 min
3. Foam Roll Lateral Quad – 10-15 seconds per region – Just roll hamstring and quad like you normally would, but edge in on that lateral quad! ~ 30 seconds
Good luck!
Get more information about NFPT Personal Trainer Certification >>
___________________________________
[sc name=”anatomy” ][/sc]
References
https://www.physio-pedia.com/Iliotibial_Band_Syndrome
https://news.harvard.edu/gazette/story/2015/08/understanding-the-it-band/
https://www.physio-pedia.com/Iliotibial_Tract#:~:text=Extremity%20Myofascial%20Chains-,Description,pelvic%20stabilisation%20and%20posture%20control.


