Those pesky ball-and-socket joints going every which way can really confuse matters of movement, even for personal trainers, can’t they? The hip, like the shoulder, can move in all planes of motion powered by any number of the 17 muscles that are responsible for its joint actions (21 if you break up the three major glutes into their eight sections!). You may have already studied up on hip adduction and flexion, but hip rotation and abduction are other matters.
I decided to lump these two actions together since there is so much overlap between them. Add hip flexion to the mix (which makes an appearance here) and now you’ve really got a lot to sort out!
Hip Internal Rotation and Abduction Muscles

Gluteus medius
Glute medius is located on the lateral pelvis, between the two spiny processes: anterior superior iliac spine (ASIS) at the front of the pelvic bones and the posterior superior iliac spine (PSIS) on the back. It attaches to the greater trochanter and fans out into insertion points along the iliac crest.
This conundrum of a muscle does it all: Abduction–and 60% of all hip abduction at that–accomplished mainly by the middle fibers of this three-sectioned muscle. But it doesn’t end there! The anterior fibers help internally rotate and flex the femur, while the posterior fibers extend and externally rotate the femur.
Test its function by placing the thumb of your right hand just lateral to the PSIS and the four fingers just below the ridge of your ilium on your lateral hip. Lift your right leg straight out to the side with your toes pointed straight ahead. Now, rotate your femur medially by pointing your toes inward.
You will feel the muscle under your four fingers contract slightly more. Then, rotate your femur laterally by pointing the toes away from your body and slightly extending the leg behind you. Your thumb should feel the posterior fibers of glute medius contract more strongly.
Tensor Fascia Latae (TFL)
Don’t let the word “fascia” fool you here. TFL is indeed a muscle, but it invests into the IT Band from the ASIS instead of into another bone. Oftentimes when people have problems with the IT Band the problem is really with TFL, or even the glutes which also invest into the ITB. When the TFL is short and tight, it may contribute to excessive tibial external rotation and/or anterior pelvic tilt.
This bugger of a muscle is hard to connect with since it is also responsible for a few contradictory motions. The TFL performs hip abduction, but also flexes and internally rotates the hip. Women with wide-set hips tend to have short TFL’s.
Gluteus Minimus
Glute minimus is deep, but also fans out from the greater trochanter to the iliac crest, like glute medius. It has two sections with separate insertion points: one that attaches to the anterior portion of the ilium and one that attaches more laterally.
The actions of glute minimus are closely aligned with the TFL and glute medius being situated beneath or inferior to them. It’s a hip stabilizer and is best at performing hip internal rotation, and also at decelerating hip adduction (basically, fighting against the adduction of the pectineus and other anterior adductors). Think of it as a synergist of hip flexion and abduction: it assists in those actions but isn’t primary.
Because of it’s deep location, it’s difficult to palpate this muscle in action.
Working Together
So to feel these muscles in their most contracted position place the fingers of your left hand on your left hip just below your ASIS and place your thumb just lateral to the PSIS. Keep your weight shifted into your right foot so that the muscles you’re palpating don’t work to stabilize the left hip. Turn the toes of your left foot slightly away from your body and lift the leg slightly out to the side into abduction. Then rotate your toes inward to internally rotate your femur.
The three muscles above are all working together to perform this motion. You should feel all the muscles under your fingers tighten up!
Hip External Rotation and Horizontal Abduction Muscles
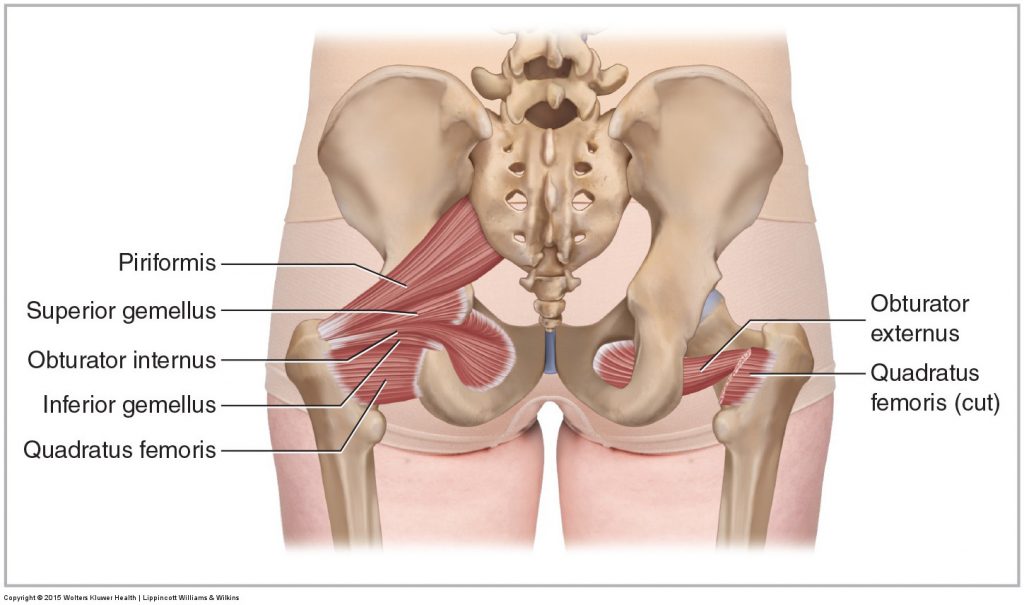
Deep Rotators
- Piriformis: This is the muscle that is most ubiquitous in terms of hip external rotation. The piriformis originates deep in the pelvis and sacrum and attaches to the medial aspect of the greater trochanter, sharing tendinous attachments with both gemelli and obturator internus.
By observing this anatomical illustration it’s not hard to imagine the action piriformis takes when standing (in slight hip extension): when it contracts and shortens you get hip external rotation.
But now imagine that the hip is flexed. Hmmm…with the knee raised up directly in front of you, the hip in 90 degrees of flexion, piriformis now is stretched out over the lower aspect of the ilium, i.e. lengthened. So if the piriformis is long in this position, what action will it perform when it contracts and shortens?
Horizontal hip abduction! (That’s what happens when you flex your hip and move your knee out to the side) Now for the other tiny rotators…
- Gemelli (superior and inferior): Extending from ischium to greater trochanter, both perform hip external rotation and horizontal abduction.
- Obturator internus: Also hip external rotation and horizontal abduction.
- Obturator externus: Now things get a little interesting. Take a look at the illustration above again and check out obturator externus on the right side. Instead of passing behind the ilium like all the muscles above it passes in front of it, but still attaches to the greater trochanter, just a little lower than the others. So what happens when this muscle shortens while standing up? It’s still a synergist of external rotation like the others but, instead of horizontal abduction, it is more likely to assist in adduction, by sort of hugging the proximal end of the femur closer to the midline of the body.
- Quadratus Femoris: Same goes for QF…it is short, square, and attaches from the greater trochanter to the ischium.
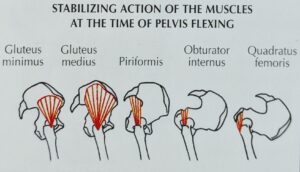
Hip Rotation Harmony
As tiny muscles, these deep hip rotators are more responsible for hip stabilization than the bigger muscles that surround them. This could be why, when the glute medius and glute maximus are inhibited or not performing all that well in everyday activities or exercise performance, the piriformis and all of its little helpers tend to become overactive to compensate.
This can become most clear during a squat when the knees bow out towards the pinky toes instead of staying aligned with the second and third toe of each foot. When the knees bow out towards the outer foot at the bottom of the squat (horizontal abduction!) you can assume that the deep rotators are short and overactive and need some releasing and stretching. Beyond that, getting the bigger glute muscles on board with activation and integration with movements will help solve that synergistic dominance of the deep rotators.
Same goes for someone who has a posterior pelvic tilt: These muscles are likely to be tight and overactive.
But what about people who have an anterior pelvic tilt or whose knees bow in during a squat (horizontal ADduction!)? As you might have inferred the deep hip rotators are long but almost never are they underactive. As mentioned above, these guys have to stabilize the hip and they really can’t get away from that responsibility.
Long, overactive muscles might have trigger points and need to be released and calmed down, but they don’t need to be stretched.
In these scenarios, the deep rotators are doing the dirty work for the weaker glute medius and are probably getting a lot of help from an overactive TFL. Focusing on glute complex activation and strengthening is the best approach after releasing these overactive hip rotators.
[sc name=”masterfitness” ][/sc]
References
https://brookbushinstitute.com
https://en.wikipedia.org/wiki/Piriformis_muscle
By Anatomography – en:Anatomography, CC BY-SA 2.1 jp, https://commons.wikimedia.org/w/index.php?curid=27660224